
For most patients, the buzzing sound is unpleasant - it gets under the skin and you can't stop thinking about it because it reminds you that you are lying in a mysterious tunnel that is investigating you in some way. But for Petra Jiříčková, head of the Multiscan radiology department in Pardubice, it's a tune she's long been used to. "It's kind of rock'n'roll," smiles the Pardubice doctor as she listens to the typical sound of the MRI scanner just outside her door. "I get rather nervous when I don't hear any sound, then I wonder why we don't investigate. It's the same with an MRI or a computed tomography (CT) scan as it is with airplanes, they too must not be on the ground unnecessarily. That's why we go seven days a week and usually on holidays," he adds.
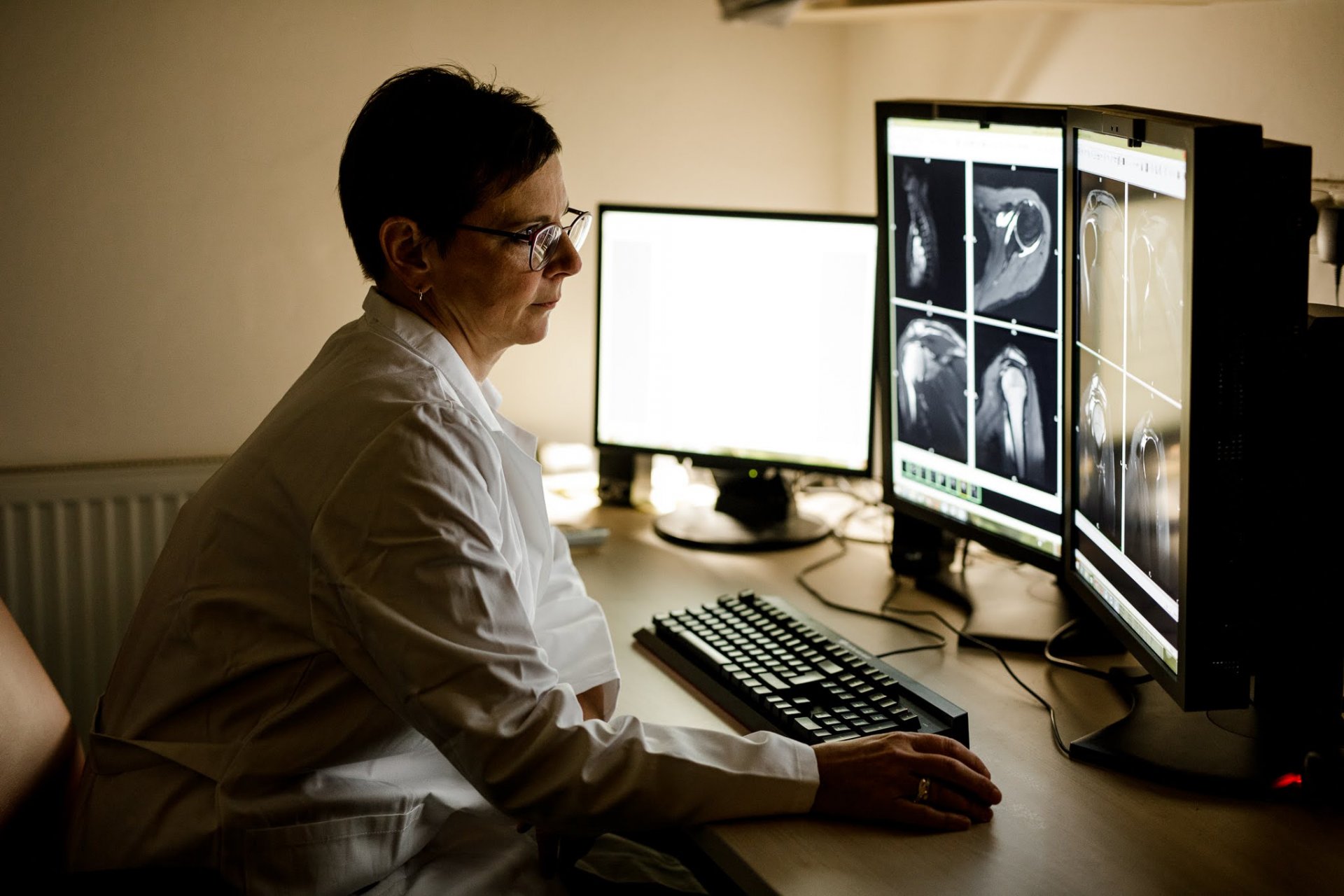
We are just outside the centre of Pardubice in one of the best-equipped diagnostic centres in the Czech Republic. Over 21,000 people a year are examined here for MRI and CT scans alone. Most of them are patients who do not suffer from any fatal disease, but some of them are cancer patients. It is here that their road to recovery usually begins, and it is thanks to doctors like Petra Jiříčková, who spend long hours in the dark squinting into monitors and describing the changes in their bodies, that their chances of being cured grow. Nowhere else do you realise the distance medicine has travelled as much as here.
Petra Jiříčková knows the human body from the inside like few others. As she says herself, there is currently no place in it where we cannot look with the help of sophisticated instruments. Yet she usually does not see her patients in person and they do not know her. But when you talk to her, a fascinating world opens up where nothing is impossible thanks to the combination of cutting-edge science and medicine.
"I got into it myself by accident, because it was actually a bit left over from school. But I'm a technical type, so I enjoy it. And today I've been doing it for almost 30 years," she smiles.
How have your opportunities improved over the three decades?
Tremendously. When I started, CT scans were only in a few hospitals. We got a single-row CT scanner in Cologne then, which is ridiculously small by today's standards, and it was glorious. And then a little later came MRI. First it was in the big cities and then it spread further afield. And the spectrum of diseases it's used for has changed. In the beginning, there was a lot of consideration about who to send for an MRI, it was more for more serious diagnoses. Today, it's used for minor ailments.
A top neurosurgeon, Vladimir Benes, recently told me how better diagnostic equipment has completely changed his field, because without it the surgeon didn't know what he was operating on until he started.
And it's a change not only for the doctors, but for the patients as well. When I started, I was still in the days of perimyelography...
What's that?
It was sticking a needle into the spinal canal, injecting a contrast agent, and then imaging the patient to see where the disc prolapse was. There was no other way to tell then, but nowadays it's not done anymore, or very rarely, because we can see it beautifully without having to torture the patient.
What else has changed?
It used to take ten minutes to do a CT scan of the brain, now it's seconds. Everything has become faster and more precise. Back then, they used to take ten-millimetre layers, whereas now the machines can take layers under one millimetre.
What do you mean by that?
Both CT and MRI will show you the area being examined in individual layers. And it makes a difference if you have a layer that's one millimeter thin or ten millimeters thin. We look at layer after layer, looking for what doesn't belong there. And the thinner the layer is, the more accurately we can assess.
What's the difference between a CT scan and an MRI? A lot of patients are confused.
A CT scan uses X-rays, which are picked up by detectors as they pass through the body and from that the computer constructs a final image of the area being studied, whereas an MRI uses a strong magnetic field and the computer calculates how the different tissues behave as it changes.
What is each method used for most?
Each has its advantages. Magnetic resonance imaging is great for imaging soft tissue, which then doesn't even need a contrast agent. With CT, on the other hand, soft tissue is more of a bland grey, so MRI is always better at this. CT is better for bony structures, plus it has the advantage of being a shorter examination. The whole body can be examined in a few seconds, but with MRI it takes minutes for one sequence and half an hour for the whole examination.
You have some of the best equipment in the country. What are you most proud of technologically?
We have an MRI with a magnetic field strength of 3 tesla here, so I guess that's what I'm looking forward to, because it's a really high-end machine. I would say we are one of the top in the Czech Republic.
Is there any other place in the human body that you can't see, in layman's terms?
In a combination of several methods we are able to see just about anything. It is possible to perform, for example, tractography with magnetic resonance imaging, which is incredible. We can image a lot of things, but the question is whether we know what to do with it.
What do you do most in Pardubice?
We perform a wide range of diagnostics in MRI, starting with examinations of the brain, spine, musculoskeletal system, we examine the abdomen, pelvis, prostate, cervix, rectum. We also perform heart examinations. We also have ultrasound, where we primarily examine the abdomen, blood vessels, heart, soft tissue. And last but not least, we have x-rays, where we take mostly pictures of the chest, spine, joints.
We're sitting at your computer right now, where you're describing what your machines find. What's on your monitor now?
This is a lady with a vertebral fracture that was treated with a vertebroplasty. She broke the covering of the adjacent vertebra, which happens occasionally. Plus, she's got advanced degenerative changes there. The machine exam takes 20 to 45 minutes. Depends on the description... it could be five minutes, it could be 20 minutes.
What's the worst part of the diagnosis?
A relatively long examination is, for example, an enterography, which is an examination of the small intestine, but that's because the patient has to drink for a long time before the examination. Generally cancer patients tend to be more difficult, and for them the examination is usually associated with the administration of a contrast agent. And it's always about how well the patients cooperate.
What proportion of your patients are oncology patients?
It's 90 percent for CT scans, but for MRIs it's only 20 to 30 percent. That's where neurological and musculoskeletal tests come in.
But the cancer patient journey starts with you, right?
We don't determine the histology of the tumour, but our examination allows the clinician to choose the optimal course of treatment. They can see how big the tumor is, if it's growing, if there are metastases in the body. This, together with the histological result, is then used as a basis for treatment planning. So, yes, we are key for oncologists.
Does better diagnostics help in cancer treatment?
I think we have a role in this because we are able to image smaller tumours at earlier stages. We're able to see metastases in the brain that are several millimetres in size, which wasn't possible before. So that makes it possible to administer treatment quickly and relatively early.
What types of tumours do you see most often? Or rather, under the machines?
In MRI, it is primarily prostate, rectal, brain, some types of breast cancer and metastases.
Are you seeing anything more often than you used to?
When I was studying and someone had two types of primary tumors at once, it was already very unique. Nowadays, you find patients who have three or four types of tumors, and it's not that uncommon. Like an ovarian tumor, a thyroid tumor, and a skin tumor. That didn't used to happen much. And I don't think it's just that we couldn't diagnose it before.
How do you clear your head when you're doing this kind of work?
I go for a walk with the dog, a run or a bike ride. You can't admit it too much.
You mustn't admit it, but patients come back to you for check-ups, so you're always seeing them.
It's true that the shifts where you describe some improvement are better. But there are shifts where I've described progression of findings several times in a row, and it wasn't pretty. But most of the time I can't even put a specific face to the names because I haven't seen the patient in person, which helps me keep my distance.
You don't know a patient by their face, but you have to remember some stories by their names, right?
That's true, I do follow some stories. And I'm always happy to write that the findings are getting better. Fortunately, there are quite a few patients like that.













{kind=link}
{kind=link}